Information about metabolic performance diagnostics
What does “Performance Diagnostics” mean?
There are two main applications for performance diagnostics
Control of exercise intensities to optimize an endurance training procedure
Performance measuring, monitoring, and competition predictions (out of competitions)
(1) Control of training intensities
Both high-performance athletes and health sports enthusiasts usually share the desire to improve their physical fitness and athletic shape through training. It is particularly important to avoid overloading during training, on the one hand— and not to waste time unnecessarily and without effects in sports. Endurance performance diagnostics should help to find the golden mean and thus make the training as efficient as possible.
Training load and its determinants
Training load is primarily influenced by two key factors: training volume and training intensity. Generally, a higher training volume necessitates lower intensity, while increased intensity requires a reduction in volume. Training load can be understood as the product of these two variables.
Individual differences play a critical role in managing this balance. Some athletes are more resilient and can tolerate higher loads, while others may respond better to increased intensity or greater volume, depending on their physiological makeup and specific goals—whether targeting competitive performance or general fitness.
Given this variability, accurately determining training intensity is essential. However, athletes often struggle to assess training intensity objectively on their own. Performance diagnostics can provide a reliable foundation for effective training planning, ensuring that intensity levels are tailored to the athlete’s needs and capabilities.

Optimize endurance training
Finding the efficient training intensity in endurance sports without help is not
easy. Performance diagnostics supports with the approach of training control. In the
high-end zone, a whole range of different training load intensities can be
objectively identified and controlled with performance diagnostics—not just one
single ideal training zone.
Simple rules don’t work
Recommendations on the intensity of endurance training are still frequently derived from simple rules of thumb based on maximum heart rate values or the age of the athlete in elite sports, rehabilitation, and health-related prevention. Often, algorithms are also used in smartwatches or fitness-watches to derive training recommendations from the general heart rate behavior (Fig. 12).
Important
Heart rate values vary significantly individually in relation to the real metabolic stress (see Fig. 12).
Tip
The individual feeling of exertion can sometimes mislead exercisers—some people hardly feel exerted while they are already overloaded. And vice versa.
Performance diagnostic stress tests can provide greater certainty regarding the actual individual heart rate responses during physical exertion. Conducting performance diagnostic tests in the lab or under field conditions allows for the objective measurement of the relationship between individual heart rate and performance data to the actual intensity of physical exertion.
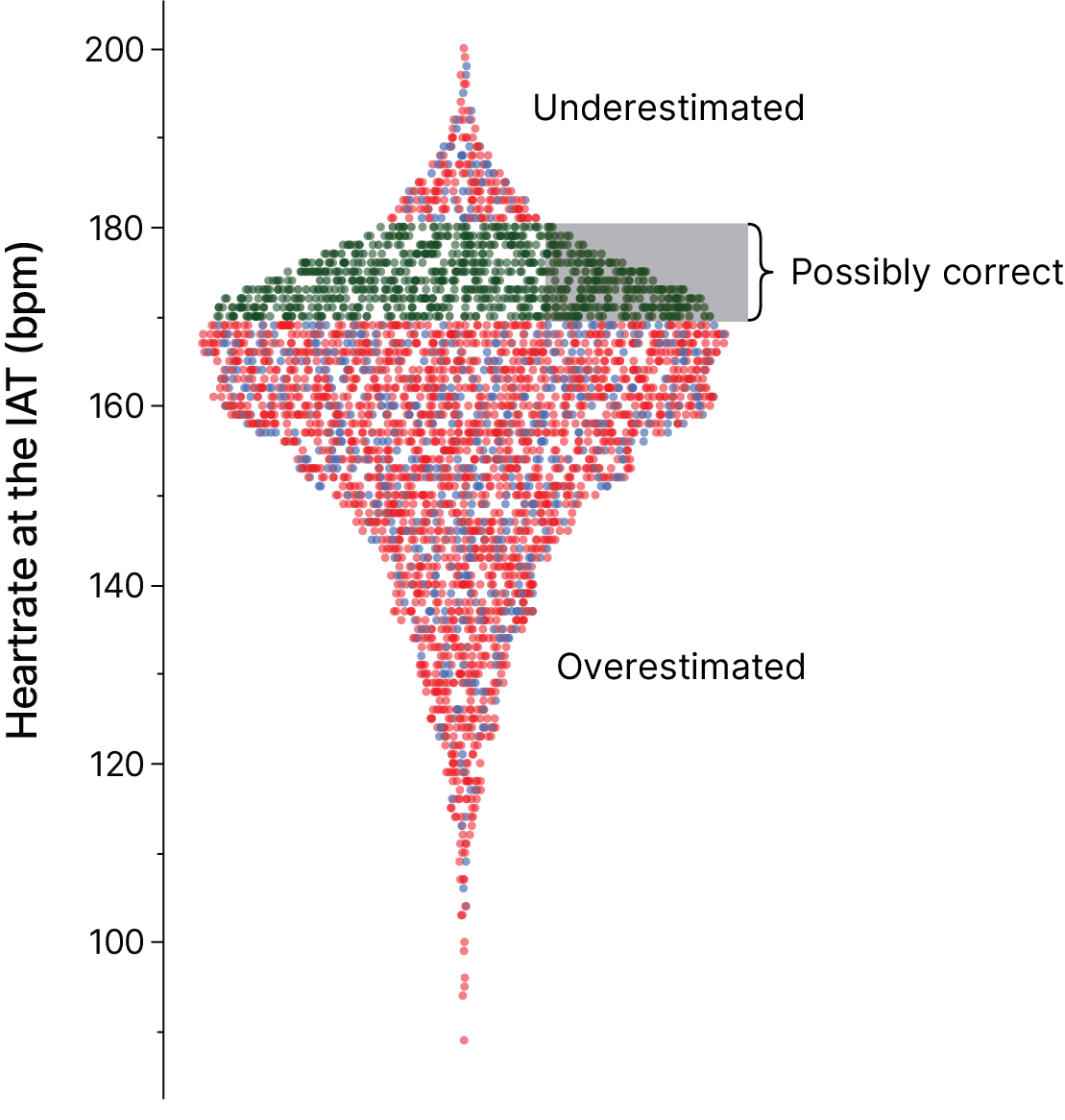
The most precise estimation of exercise-induced strain can currently be achieved by measuring the lactate concentration in capillary blood. Lactate concentration increases with the proportion of the so-called Anaerobic Glycolysis in energy supply and is thereby an objective measure of the level of exertion—regardless of the individual perception of exertion.
(2) Measuring endurance performance
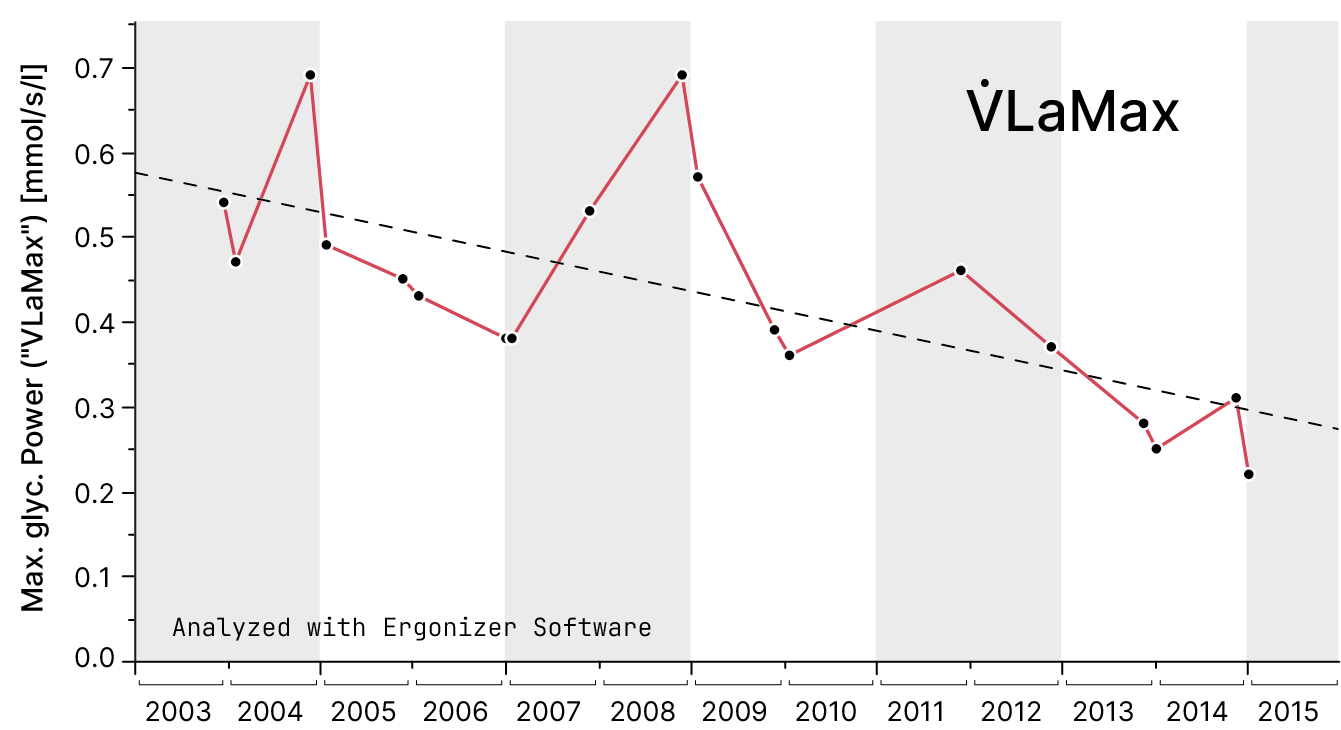
Another important area of application for performance diagnostics is the reliable identification of specific endurance performances and the analysis of the various components in diverse settings. In the time course, it can be important for health athletes up to Olympic athletes alike to receive feedback on the positive effects of their training. Successful training leads to a positive improvement in fitness. Identifying this reliably and with reasonable effort is the task of performance diagnostics. In modern application, many new metrics of performance diagnostics are applied to lactate diagnostics (e.g., Fig. 13).
Methods of metabolic performance diagnostics
Physiological anchor points and the famous breakpoint Anaerobic Threshold”`
As an anchor point for performance diagnostics, various concepts for determining
the so-called Anaerobic Threshold have been developed. The “Anaerobic
Threshold” is thereby the oldest and most famous concept for a breakpoint from
increasing lactate concentration against the increasing exercise intensity. From
the scientific viewpoint it is not fully clear, how is the first describer of
the concept. In most of the English sources Wasserman et
al.[1] provided the first an distinctive definition.
In some other sources, the Cologne scientist Wildor Hollmann is named as the
inventor of this distinctive point. However, Hollmann’s breakpoint terminology
(Point of Optimal Respiratory Efficiency) differs from that of
Wasserman and Whipp[1][2].
The concept of the Lactate Threshold (LT)
according to Wasserman and Whipp[1] serves as another reference for
endurance training recommendations in Ergonizer. Despite the similarity of
this term to the “Anaerobic Threshold”, however, the LT denotes a different intensity of exercise: the earliest moment of an increase in blood lactate concentration as exercise continues to increase.
The LT is helpful as a metabolic reference point and
upper limit for the lowest exercise intensity for the development of long-term
endurance. The second important anchor point for determining cardiopulmonary
performance and calculating training intensities is the so-called “anaerobic
threshold”. In contrast to the original idea of LT,
a characteristic value was sought that was more representative of the practical
sports performance of near-competitive endurance intensities.
“The Anaerobic Threshold is reached at a power output above which the oxidative energy production is supported by anaerobic mechanisms. The intensity of this stress load is accompanied by an increase in lactate and the lactate/pyruvate ratio in the body.”
Decades of research have been dedicated to exploring the source of stress-related energy supply, with a major focus on British Nobel laureate A.V. Hill[3] and also Margaria et al.[4]. Characteristic of the findings at that time was the concept of a three-phase energy provision:
a) the non-lactic-anaerobic energy provision
b) the aerobic-oxidative energy provision
c) the lactic-anaerobic energy provision
depending on the intensity and duration of the exercise.
The further historical context for determining and also defining this so-called anaerobic threshold is diverse. German scientists have also made a significant contribution to the early development of the method for sports medicine and sports science. Hermann Heck and his research group are particularly credited with establishing the above-mentioned and so-called “anaerobic threshold” for endurance performance tests of athletes. Anyway, as always in these times, the term “anaerobic” has been misused in those concepts.[5]
Unlike in the past when it was thought that lactate was the consequence of a lack of oxygen in the tissue (“anaerobic”), we now know that lactate is continuously produced even when there is sufficient oxygen available. In this way, lactate can be oxidized at any time, especially during moderate exercise intensities. The working muscles not only produce lactate (especially in glycolytic muscle fibers) but also consume it (especially in oxidative fibers). Based on this so-called “cell-cell lactate shuttle,”[6] lactate diagnostics also received a completely new rationale. The so-called “anaerobic threshold” is definitely not marked by the onset of energy provision without use of oxygen (as postulated by Wasserman and Whipp[1]). Rather, an increase in the lactate concentration is the result of an imbalance between production and oxidative elimination of lactate (intramuscularly via the lactate shuttle or through the Cori cycle in the liver)[7]. Individuals with higher relative rates of lactate production may be affected by a limited endurance performance, just like individuals with a lower elimination rate via oxidation.
The fundamental principle is still part of modern performance diagnostics: The better the endurance performance of a test subject, the more the increase in lactate concentration is shifted to the “right” with increasing exercise intensity (see Fig. xx). Anyway, an increase in blood lactate concentration in healthy test subjects is completely normal and certainly not caused by any illness. The increasing exercise load (according to Wasserman and Whipp[1]) leads to a growing involvement of a glycolytic energy supply, resulting in an increase in the concentration of the metabolite lactate in the blood – if these amounts of lactate are not metabolized, e.g., as oxidative energy sources. This relationship, between blood lactate concentration and power out, is graphically represented in performance diagnostics as “lactate performance curve” and forms the basis for determining the anchor points for referencing training intensities[8][9]. The term “anaerobic threshold” or even “threshold” should thereby only be used for historical reasons or because the term is generally well known – and with caution.
Hint
By determining the “anaerobic threshold”, endurance performance can be assessed. The higher the performance at the “anaerobic threshold”, the higher the endurance performance capacity, respectively, the cardiorespiratory fitness of the person being tested.
In addition, based on the “Anaerobic Threshold,” a classification of training intensities for endurance training was made. The “Anaerobic Threshold” thereby serves as a reference point for increasing endurance capacity: the higher the endurance performance capacity, the higher the training work load can be set without triggering an overload reaction.
While it is undisputed that the individual lactate increase vs. performance (“lactate curve”) is a reliable measure of actual performance, it is not clear whether the conventional reference points for determining the anaerobic threshold are actually capable of reliably determining the position of the lactate curve. Over the years, various proposals for anchor points, each of which has its own advantages and disadvantages (Tab. 1). The main criterion for selecting one of these reference points for determining cardiopulmonary cardiopulmonary fitness or to control the training are, however, the reproducibility rather than validity.
You can’t do a competition every day
Maximum performance, but without maximum exhaustion
Performance diagnostics can be used not only to control training, but to objectively assess performance. For this purpose, Ergonizer offers prognosis and analysis tools that provide precise information on dynamic performance—from simple exercise diagnostics—for a variety of specific types of exercise.
In competitive sport, this has the advantage that a performance diagnostic test is typically less stressful than a “real” competition. In other words: with performance diagnostics, you can predict what you are able to achieve in a marathon—without actually taking part in a real marathon race. In other words, without the severe exhaustion that is generally to be expected after a marathon.
Performance diagnostics?
The term “performance diagnostics” is often used in sports medicine or sports science as a synonym for the objective measurement of cardiopulmonary performance, cardiopulmonary fitness or even endurance capacity [2]. Other factors of physical performance such as strength, coordination or speed thereby seem to be of less interest. One reason for this peculiarity may lie in the outstanding importance of endurance as a predictor of life expectancy and mortality[18]. In addition, endurance exercise is considered to be the most effective intervention for targeted health-promoting calorie expenditure.
But even more in many comptetive sports, endurance performance is a necessary (e.g., in many game sports) or even necessary (e.g., in long-distance running, triathlon or cycling) prerequisite for high sport-specific performance[19].
Multiple indications for performance diagnostics
Performance diagnostics serve a wide range of purposes, both clinical and non-clinical. In clinical settings, they are essential for assessing cardiopulmonary fitness, diagnosing potential health issues, and guiding rehabilitation programs. Non-clinically, they are invaluable for athletes and fitness enthusiasts aiming to optimize training, monitor progress, and achieve specific performance goals. This dual applicability highlights the versatility and importance of performance diagnostics in promoting both health and athletic excellence.
Possible uses of endurance performance diagnostics
Measurement of endurance performance and cardiopulmonary fitness in athletes and normal individuals (performance diagnostics)
Preparation of training recommendations for the development of endurance performance (training control)
Training prescriptions and follow-up diagnostics in rehabilitation
Specific performance prognoses for competitive endurance sports
Scientific characterisation of test subjects in terms of motoric abilities
Determination or progression assessment of functional impairments in severe chronic internal diseases
Diagnostics for suspected myopathy or mitochrondriopathy
Preoperative evaluation for special diseases (e.g. for the question of heart transplantation or partial lung resection) usually in combination with measurement of maximum oxygen uptake
Expert opinions on the objectively measured performance of test subjects
Occupational medical examinations and expert opinions
The multi-stage test, a universal test principle
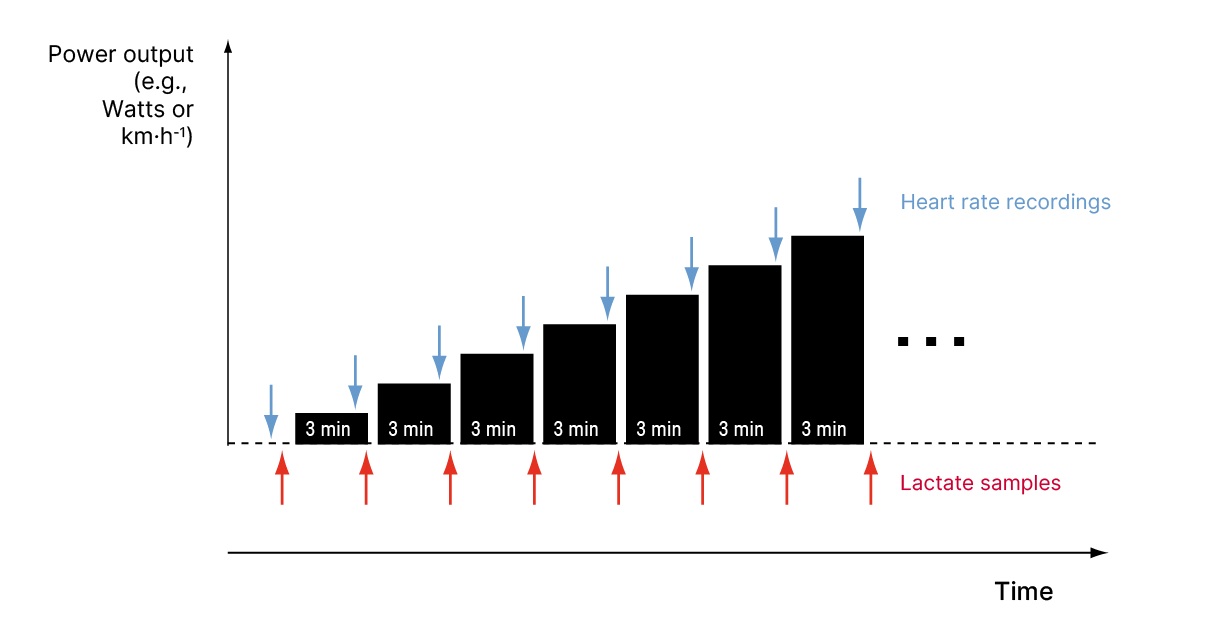
To determine the “anaerobic threshold” and other reference data for endurance performance, the blood lactate concentration is plotted against the performance achieved in the form of a so-called “lactate performance curve”.
The test procedure is usually carried out as a so-called multi-stage test (Fig. 14). This means that with each stage of constant duration, the performance is increased by constant step increments.
Power calculation of the last step in a multi-stage test
If the test was ended prior to a full step duration, e.g., due to exhaustion of the subject, the maximum power output (\(P_{max}\) ) is calculated as a percentage using this equation (1):
whereby \(t\) is time duration and \(P\) is power output. More specifically, \(P_{penultimate\ stage}\) is the power output on the penultimate stage, \(P_{increment}\) is the increase in power output on each stage, \(t_{last\ stage}\) is the duration of the last stage, and \(t_{preset}\) is the target for the total duration of all the stages. So if, in a multi-stage test with a duration target (\(t_{\text{preset}}\)) of 3 minutes, \(P_{increment}\) was 50 watts and the last stage at 350 watts could be sustained for one and a half minutes (\(1.5\ min\)), the result is given in (2):
This calculation is performed automatically by Ergonizer. However, drawing lactate curves by hand would not only be tedious but prone to error: different examiners naturally apply different criteria for the interpolation and evaluation of such a curve. Even the use of spreadsheet or non-specialized statistics software, for example, does not provide a robust and natural measurement result.
Important
An exercise test up to maximum exhaustion without medical supervision may only be carried out on healthy persons or after a positive health examination.
Ergonizer evaluates and clearifies test results
Ergonizer automatically creates robust evaluations of all relevant results and calculation data from your exercise tests, independent of the examiner. In the resulting automatic evaluation of the general performance data and the so-called “Anaerobic Threshold”, the program calculates a list of all relevant training zones for individual specifications that are important for the supervision of successful endurance training.
Warning
A performance diagnostic examination is in no way a substitute for a sports medical health examination. In the medical context, however, performance diagnostics is very often very often offered as an additional (also medical) service.
Various types of exercise with lactate diagnostics
Lactate diagnostics can be carried out using a wide range of different types of exercise. Most frequently, such tests are carried out on the bicycle ergometer, and by running or walking tests on treadmill ergometers. The use of various other special exercise modes, e.g. rowing, canoeing, hand cycling, hill running, x-skiing, or swimming, are carried out with the aim of achieving the highest possible degree of conformity with the various sports and forms of movement. Hand crank ergometry is also frequently used to assess patients with pathological impairments of the legs.
Additional application options for special load modalities in field tests, such as fencing, are also possible[20]. However, note that specificity often means that the standardization of exercise intensity is abandoned. For example, in treadmill tests with cross-country skiers, the running speed cannot be converted into a valid physical power output. Furthermore, in rowing and canoeing ergometries, or in field tests, there is no technical option of automatically regulating performance. The test subject must therefore follow an external power target themselves, which requires a certain amount of practice and familiarization with the test.
The transfer of results between e.g., cycling and treadmill ergometry or other types of exercise is only possible to a very limited extent due to significantly different locomotor demands[21][22]. In general, the more ambitious the competitive sporting commitment of the person being tested, the more specific the ergometer should be selected. Long-distance runners or soccer players should ideally be tested on a treadmill, cyclists on a bicycle.
Usually, treadmill ergometry results in a slightly higher cardio-circulatory load than cycling and can also be used for people without cycling experience. However, it is challenging to carry out capillary blood samples or ECG recordings directly during a running exercise; why treadmill exercise must be paused briefly after each exercise stage. Tests on the cycle ergometer, but, can be carried out without pauses. Also, simultaneous spiroergometry (respiratory gas analysis during exercise) can be interpreted more reliably on the cycle ergometer than on the treadmill due to the lack of pauses between the stages.
The specified performance on the ergometer is also subject to fundamental quality criteria as a measured variable for performance diagnostics and must be adjusted through regular device calibration. Field tests, on the other hand, pose the challenge of precisely measuring and controlling performance using, for example, GPS for running or pedal force measurement cranks for cycling.
Important
For reliable data interpretation, regular calibrations of the ergometry device and the measuring device for the lactate concentration are highly recommended.
Practical recommendations for multi-stage tests
The most frequently used specification for the stage duration in multi-stage tests is 3 min. Tests with a different, but continuously constant duration (e.g., 2 or 5 minutes stage duration) is comparable with each other. However, different stage durations produce different results in lactate diagnostics—without the information gain increasing, e.g., if the stage duration is extended. The subsequent extension of the total test duration may result in premature termination of the exercise in some test subjects.
Time-dependent redistribution processes are also responsible for the fact that the maximum blood lactate concentration cannot be recorded directly at the end of the test, but often only a few minutes after the end of the exercise, depending on the total duration and intensity of the test. This means that several post-exercise values must be measured during the course of the test (e.g. in the 1st, 3rd, 5th and 10th minute of post-exercise) in order to reliably record the real maximum value for the lactate concentration.
Hint
A multi-stage exercise test must include at least 5 steps and a total duration of at least 15 minutes for healthy athletes. More stages improve the accuracy of the interpretation by Ergonizer. Anyways, too many stages and a too long total test duration reduce it again. If the respondent is not strong enough to complete at least 5 steps in the regular test protocol, you should consider reducing the duration of the steps (2 min).
A correct interpretation of the increase in lactate during exercise requires a sufficient number of individual exercise levels and therefore measuring points. But, an enough number of measuring points in the lowest load range is also necessary to record the LT.
Important
Treadmill tests on healthy and fit subjects should always be started at 6 km/h rather than at 8 km/h. If a person appears really to be too fit for 8 km/h, an additional 3-minute step at a low load intensity will certainly not bother them. However, the accuracy of the evaluation will improve vastly.
As the performance capacity of the test person is naturally not yet known before the test, it is advisable to extend the start of the test to the lowest possible performance. For example, even very fit runners can run at a speed of 6 km/h without any problems, while people with performance limitations will already have a certain increase in lactate concentration at 8 km/h.
The special requirements of lactate diagnostics therefore result in recommendations for exercise protocols that deviate in part from the other clinical-medical guidelines (Tab. 2). This applies, for example, to the simple exercise ECG (2-minute step duration, higher starting power to avoid excessively long tests) and in particular to the performance of spiroergometry (ramp test). If the simultaneous performance of spiroergometry and lactate diagnostics within a test sequence is desired, compromises must be made in the exercise protocol in favor of lactate analysis.
Group |
Start |
Increment |
Step Duration |
|---|---|---|---|
Cycling Ergometry |
|||
Clinical patients |
20 W[23] |
10 W |
1 min |
Outpatients and rehabilitation sports |
25 W[24] |
25 W |
2 min |
Healthy normal persons |
50 W |
25 or 50 W |
3 min |
Recreational athletes |
50 W |
25 or 50 W |
3 min |
Competitive athletes |
50 W |
50 W |
3 min |
Cyclists (BDR) |
80 W |
20 W |
3 min |
Treadmill (Walking with constant speed) |
|||
Clinical patients (Walking test) |
0% gradient at 2, 4, or 6 km/h constant speed |
2.5% or 5% gradient |
2 min[24] |
Outpatients and rehabilitation sports (Walking test) |
0% gradient at 2, 4, or 6 km/h constant speed |
5% gradient |
3 min |
Treadmill[25] (Running with constant gradient) |
|||
Healthy normal persons (Walking test) |
4 or 6 km/h, ~1.5% constant gradient |
2 km/h |
3 min |
Recreational athletes (Running test) |
4 or 6 km/h, ~1.5% constant gradient |
2 km/h |
3 min |
Competitive athletes (Running test) |
6 km/h, ~1.5% constant gradient |
2 km/h |
3 min |
Field test running (e.g. 400m track) |
|||
Normal people and athletes (Running test) |
300m (6 km/h) or 400m per 3 min (8 km/h) |
100m per 3 min (2 km/h) |
3 min |
Rowing ergometry |
|||
Competitive athletes |
50 or 100 W |
50 W |
3 min |
Measurement of the capillary blood lactate concentration during exercise
The most important application of our software Ergonizer is based on the graphical-mathematical evaluation of lactate in the capillary blood during standardized physical exertion. For this purpose, small amounts of blood must be taken at regular intervals during an exercise test (multi-stage test).
Hint
Blood sampling from the fingertip is not recommended for various reasons for exercise tests. It is much better to take capillary blood from an earlobe.
Taking blood from the finger or the earlobe?
Even if it may seem sensible for practical reasons to take the blood sample for the lactate measurement from the finger instead of the earlobe, there are many arguments against it.
The most important argument in favor of the earlobe as the sampling site is that this is the only place to obtain the “right” blood for analysis: The earlobe is supplied with arterial blood directly from the heart—without any detours or interference from working muscles or larger organ compartments.

The earlobe blood corresponds to the mixed venous blood stream, i.e. it represents the lactate concentration that is mixed from all compartments of the body, meaning that clean lactate values are only obtained from the earlobe during exercise, but not from the finger.
At the finger, lactate is either too high or too low
Depending on the type and intensity of exercise, lactate values from the finger are either too high or too low. On the one hand, values are measured incorrectly and too low when the arm muscles are rather relaxed (e.g. during running slowly) and therefore absorb lactate from the body. This amount of lactate is then missing at the fingertip for a representative measurement.
Conversely, you will get incorrectly high values if the arms are under heavy strain, e.g. when pedaling intensively on the cycle ergometer with strongly pulling on the handlebars – always if relevant portion of work done with the upper extremities. This effect is particularly extreme when exerting yourself on the rowing ergometer, swimming or cross-country skiing.[26][27]
Preparation and temporal stability of lactate samples
Keep your samples cool
The stability of the lactate concentration in blood samples depends on the post-processing of the samples - over time, this may result in incorrectly high lactate values from ongoing glycolytic processes. Non-haemolysed whole blood samples show a significantly stronger upward drift than haemolysates due to redistribution processes and vital glycolysis in the erythrocytes. If testing large numbers of subjects or athletes as in, e.g., field tests synchronously, cooling of the samples with wet ice or ice packs might be an option for better stability. Hemolization in combination with cooling improves the stability even more.
Attention
Cooling of lactate samples to 4°C (39°F) increases the stability of lactate values significantly.[28]
Furthermore, lactate measurements from whole blood lactate needs correction against hemolized values since the amount of lactate from inside the (intact) erythrocytes can not be registered. Nowadays, whole blood without hemolysis is mainly used in portable photometric devices, which in turn require immediate measurement, so that the problem of redistribution over time is not relevant. However, there is the described need to convert the lactate concentration with estimated consideration of the amount of lactate within the red blood cells.[29]
The use of heparinized whole blood as in BGA devices with parallel determination of the blood lactate concentration as in the critical care context is definitely unsafe due to the unclear distribution situation between the extra- and intraerythrocytic compartments and is therefore not recommended for exercise diagnostics. Measuring the lactate concentration in blood plasma is also no longer recommended for the same reasons, although many reference data from the 1970s to 1990s were still based on this technique.[30]
Hemolyzation might be an alternative
Haemolyzed samples, on the other hand, can be measured stably for about 20 h without cooling. In addition, haemolysis always makes the entire amount of lactate available for the corresponding sample volume, regardless of the redistribution dynamics described [31], so that haemolysis is generally recommended today. If an even higher temporal stability of the lactate concentration is desired (e.g. for longer excursions), the haemolysed samples can also be frozen or mixed with antiglycolytic substances (e.g. fluoride salts). However, attention must be paid here to a possible interaction of the analytical reaction with the stabilising substances.
Attention
Measured lactate results can vary significantly between hemolyzed and non-hemolyzed whole blood samples. In non-hemolyzed samples, the lactate contained within red blood cells is not accounted for, potentially leading to underestimation of the total lactate concentration. Hemolyzed samples, on the other hand, release all intracellular lactate, providing a more accurate representation of the total lactate concentration in the blood.[32]
Furthermore, no sufficient constant conversion method exist between the two.